Cardiac myxoma is a benign tumor of the heart formed by cells derived from multipotent mesenchymal cells.
The first description of a cardiac myxoma was published in 1845. For many years, cardiac myxomas could only be diagnosed at autopsy. In 1951, the first diagnosis of a left atrial myxoma was made by angiography. In 1955, the first successful removal of a cardiac myxoma was achieved.
It is the most common primary cardiac tumor, accounting for 30% to 50% of all primary cardiac tumors. It has an annual incidence of 0.5 per million people, being most common in adults aged 30 to 50, although it can occur at any age.
65% of cardiac myxomas occur in women, and 4% to 10% are familial. Although it is a histologically benign tumor, it is prone to recurrence, can develop in multiple foci, and metastasize to various anatomical locations.
What causes cardiac myxoma?
The cause and mechanism that produces cardiac myxoma are unknown. Hereditary myxomas appear at any age and with equal frequency in both sexes. They can be single or multiple, are located anywhere in the heart, and tend to recur.
In contrast, sporadic myxomas tend to occur in middle-aged women and are generally isolated tumors located on the left atrial surface of the interatrial septum. Sporadic cases have a low recurrence rate.
Mutations in genes for certain cardiac proteins have been described as responsible for the formation of cardiac myxomas in patients with familial myxoma. However, the exact mechanism that generates the tumor is unknown.
What are the symptoms of cardiac myxoma?
Patients with cardiac myxoma may experience a variety of symptoms, depending on the tumor’s size, location, and mobility. The reason for consultation may be symptoms due to cardiac obstruction, embolisms, or general symptoms.
- Obstruction of the mitral orifice by the tumor can lead to dizziness, shortness of breath, cough, pulmonary edema, and heart failure.
- Tumor embolisms can affect the systemic or pulmonary circulation, depending on the location of the tumor and the patency of the foramen ovale. Cardiac myxoma is the primary cardiac tumor that most frequently causes embolisms, and can involve any organ or tissue.
- General symptoms may include fever, weight loss, weakness, muscle and joint pain, and Raynaud’s phenomenon.
How is cardiac myxoma diagnosed?
The electrocardiogram of patients with a myxoma that does not cause hemodynamic alterations may be completely normal. However, myxoma often leads to dilation of the left atrium, which can be seen on the electrocardiogram. Some patients present with atrial arrhythmias and heart block, but these are rare.
The chest x-ray of a patient with cardiac myxoma may be completely normal. In some, dilation of the left atrium or cardiac chamber obstructed by the myxoma is observed. Cardiomegaly due to pericardial effusion, pulmonary edema, or foci of pulmonary embolism may also be found.
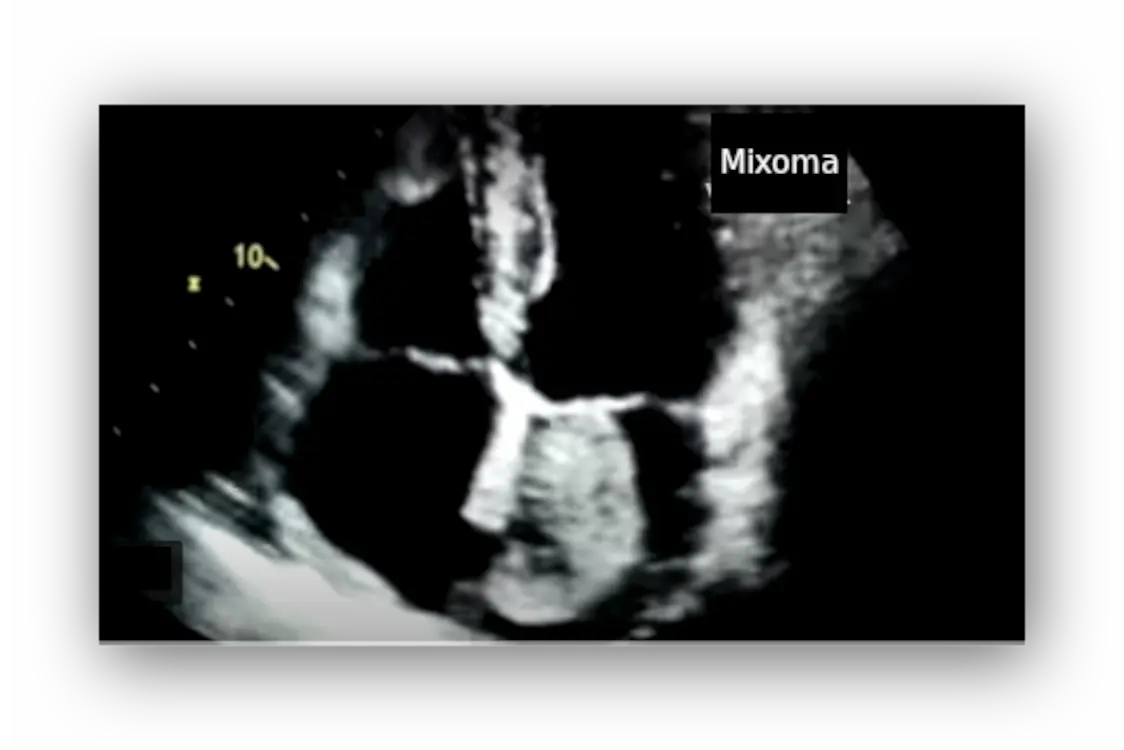
The most important diagnostic technique for diagnosing myxoma is an echocardiogram. The images obtained reveal a mass in one of the cardiac chambers, habitually in the left atrium. More than one mass is rarely found.
Myxomas are usually located in the left atrium, attached to the interatrial septum. They are typically spherical or oval, although sometimes they are polygonal or polypoid. The mass may be homogeneous or present cystic, hemorrhagic, or calcified areas.
Although myxomas may be fairly fixed, they are typically seen moving within the heart, sometimes entering the valve orifice with each cardiac contraction, eventually causing obstruction to blood flow.
In cases where the transthoracic echocardiogram does not show an image of sufficient quality, a transesophageal echocardiogram, magnetic resonance imaging, or computed tomography may be necessary.
Myxomas can also be diagnosed by angiography, but it is not commonly performed because it is an invasive technique, with its inherent risks, and can promote myxoma embolism. Catheterization is only performed if concomitant coronary artery disease is suspected.
What is the treatment for myxoma?
Myxoma treatment is surgical. Tumor resection is curative. There are no known effective drugs or natural remedies for myxoma. Medications are only used to treat symptoms or complications.
Surgery is commonly performed via median sternotomy and extracorporeal circulation, although it is also possible via thoracic endoscopy, which is less invasive, leaves less scarring, and allows for a faster recovery. During surgery, care must be taken to avoid fragmenting the tumor, which could lead to embolisms. If there is a significant valve injury, it can be corrected in the same operation. The risks are generally low, and the results are favorable.
The most serious complications of myxoma surgery are embolisms, arrhythmias, and heart block. However, the patient usually recovers well and is considered cured. In rare cases, the tumor recurs later, which occurs more frequently in hereditary myxomas.